

Ending Childhood Pneumonia #1
Exploring Problems

Hi there 👋 We (Manroop and Richa) are writing these posts to keep you all updated on our what we’re working on and our progress. Over the last week, we’ve been looking into different problems around the world in order to gain perspective and figure out which area we want to be working in over the next little bit. Our goal was to find a problem area that we felt emotionally connected with and driven to work on.

Where we Started - Child Mortality
Last week, we had a conversation with a friend, who told me about her cousin living in Pakistan whose daughter had just passed away because she was unable to receive the care that she needed. This frustrated me, and it saddened me. How is it that our world has come so far yet, children are still dying because they can’t get access to the resources they need to survive?
As a result of this, we started looking into child mortality -
From about 12.6 million under-5 deaths in 1990, to only 5 million in 2020, in the past couple of decades, we’ve made an immense amount of progress yet, these numbers are still too high.
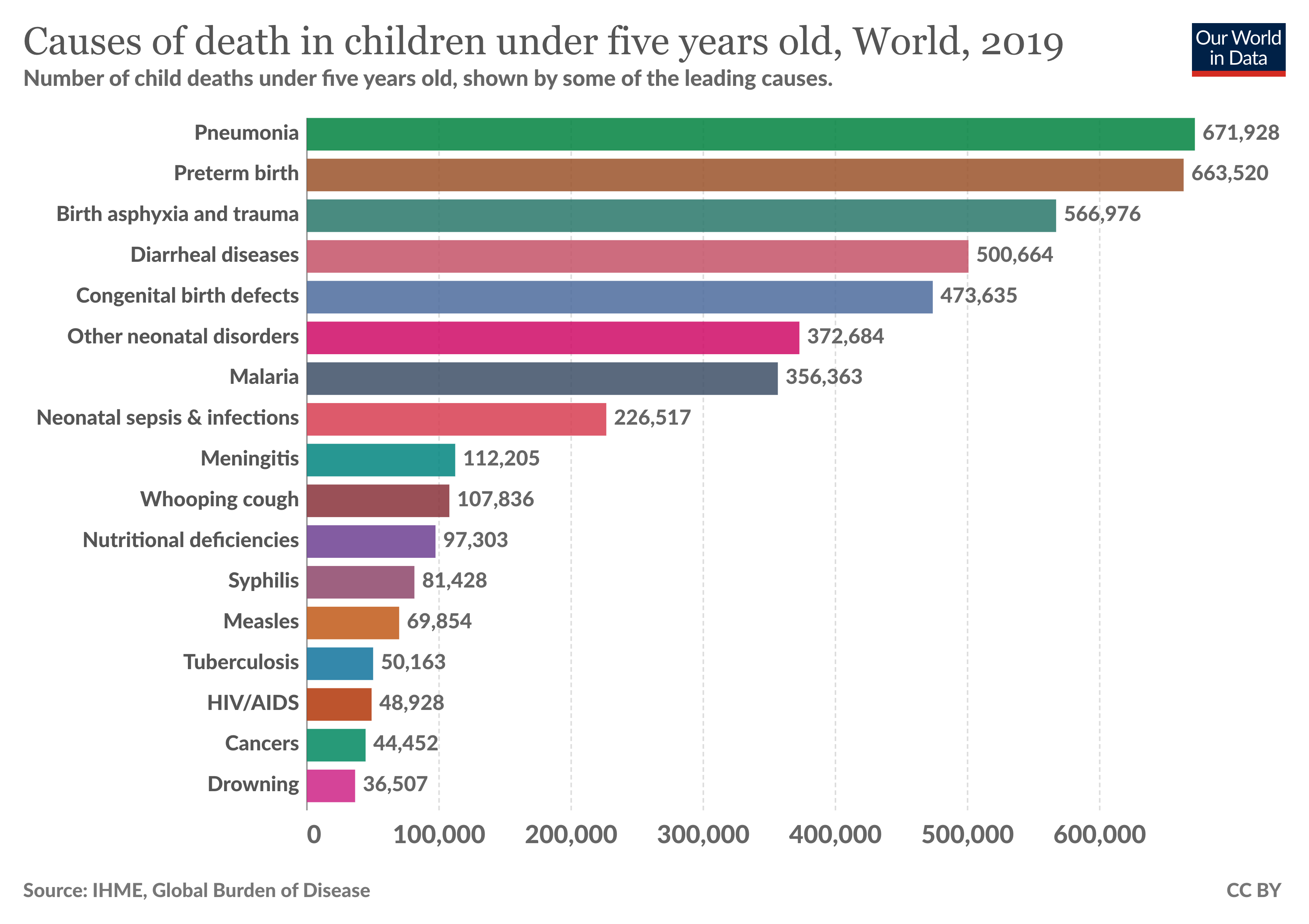
The leading cause of death for children under the age of 5 is pneumonia, accounting for almost 15% of total deaths, averaging to almost 700,000 total reported deaths in 2019.
Causes and Transmission
Pneumonia is caused by a variety of infectious agents which include - viruses, bacteria, and fungi. The most common pneumonic bacteria in children is Streptococcus Pneumoniae with the second most common being Haemophilus Influenzae.
Risk factors that have been known to lead to pneumonia include child wasting (the largest), indoor air pollution from solid fuels, low birth weight, among many other. Theses factors are more prevalent in developing nations specifically communities that are impoverished increasing the pneumonic cases occurring there.
The countries with the largest number of child pneumonia deaths are concentrated in sub-Saharan Africa as well as Asia. Democratic Republic of Congo, Ethiopia, India, Nigeria and Pakistan combined account for more than half of all deaths due to pneumonia among children under 5.
Pneumonia despite being an infectious disease is not easily transmittable, and requires close contact through air droplets to be transmitted to another person. According to a study conducted as part of the Latin America Epidemiological Assessment of Pneumococcus (LEAP), found a huge causal relationship between pneumonia and living conditions. For example, over crowding (among other factors such as sanitation, inadequate water, etc.) is a large transmission risk factor for why pneumonia has been considered a disease of poverty.
In the West, pneumonia has been almost completely eradicated proving that these deaths are completely preventable.
Current Pathways - Prevention
#1: Vaccination, the PCV13 vaccine
The PCV vaccine targets the S. pneumoniae bacteria (the most common types) and is given to children under 24 months, and is estimated to have 85% effectiveness rate. Despite this, in India and Nigeria (greatest childhood pneumonic deaths- were found to only have about 50% of one-year-olds vaccinated.
By increasing the vaccine coverage of PCV, it is estimated that approximately 400,000 lives of children could be saved each year.
#2 Breastfeeding
Undernutrition is one of the contributing risk factors to the development of pneumonia. Breastfeeding in the first 6 months of a child’s life can help reduce child undernutrition which can help circumvent the possibility of developing infectious diseases such as pneumonia. Those who are not breastfed in the first 5 months of their life have been have a 15x greater risk of developing pneumonia in comparison to those who are. In 2017, only 41% of infants were exclusively breastfed worldwide.
Treatment
#1 Access to healthcare and treatment
A delay in treating the symptoms of pneumonia (such as breathing difficulty, coughing, etc) can significantly increase the risk of mortality from the disease. Despite this, the rate of which children with symptoms are taken to a health care provider are still low across the world, with sub-Saharan Africa averaging at just 47%.
#2 Antibiotic Treatment
Antibiotics such as Amoxicillan is a low-cost and effective manner to treat penumonia. Despite this it has been found that only 1/3 children with pneumonia receive the antibiotics they need as a result of a lack of access to quality health care (whether this be as a result of misdiagnosis, stock issues, etc.)
#3 Oxygen Therapy
When a person is suffering with pneumonia, there is a possibility that the alveoli in their lungs may fill up with pus or fluid. This prevents oxygen from transfferring to their blood, and the individual to develop a hypoxemia (a lack of oxygen).
Those who develop hypoxemia have a 5x risk of dying. Oxygen therapy (providing oxygen rich air to patients such as with the use of cylinders or concentrators) is a way to treat the condition reducing the risk of death from sever pneumonia by 35%. Despite this, the need for equipment to diagnose and treat hypoxemia is a huge barrier in low-resource settings.
Oxygen therapy is an essential component to reducing deaths access to medical oxygen yet is highly inaccessible to many. Improved oxygen delivery access could translate to averting about 150,000 deaths (only pneumonia related) each year.
Pneumonia is just one of the many health issues that oxygen therapy helps to address. Therefore, we decided to shift our focus onto hypoxemia, specifically focusing on the access and quality to oxygen therapy.
Hypoxemia
Hypoxemia results when there isn not enough oxygen in the blood. It is not the first disease to develop but rather a consequence of other complications from other diseases. These may include respiratory conditions (Covid, pneumonia, tuberculosis, asthma, and more) or non-respiratory conditions (sepsis, malaria, malignacies, pregnancy, malnutrition, and many more).
High Level Breakdown of Oxygen Therapy
Oxygen Cylinders are one way of providing oxygen therapy, and is practically a tank that hold enriched-oxygen air under pressure.
Medical oxygen specifically cylinders has two main issue:
The availability of these in low income healthcare facilities extremely low (for example, it is 2% in congo, 8% in tanzania, 7% in bangladesh)
It is expensive, being approximately $40-$85 for adult per day, or for children every 3-4 days (which can be considered unaffordable for many low-income families, and has resulted in early discharges as treatment could not be conducted without the fund availability therefore, increasing mortality)
Yet, a better version of these cylinders do exist which are oxygen concentrators. Concentrators are essentially a small, robust machine that produces medical oxygen (on-demand) from the surrounding air, and can be maintained and used for years on end.
The main barriers faced with Oxygen Concentrators include:
Medical devices breaking down as a result of a lack of preventative and maintenance measures (for example, 40% of equipment in low resource hospitals is not usable)
There is a shortage of actual biomedical engineers who have the ability to fix these devices, so those that are broken tend to stay broken
The resources required to fix these devices may not be available, and “scrap-based” solutions may be difficult to implement
Service Interruptions such as power interruptions, and voltage fluctuations effect these machines as they need a constant energy supply (which may not be available in low-resource areas)
Similar to cylinders, concentrators may not be affordable for an abundance of low-income families in need
What to Expect next?
Coming up next we’ll be working on a location analysis as well as a breakdown of hypoxemia.
What causes a cold or respiratory dis-ease?
The establishment’s model of physiology FAILS under scrutiny. I’ll explain why HYDRATION and not oxygenation underpins our physiology. Understanding this destroys the sickness industrial complex and big pHARMa’s power.
A cough is a sign of respiratory dehydration not a virus or a bacterial infection. A runny nose is a sign of respiratory dehydration. Shortness of breath and difficulty breathing is a sign of respiratory dehydration. To understand this concept you need to know the extremely important difference between air and oxygen.
We breathe air not oxygen.
Air is measured by its moisture or humidity. Oxygen is measured by its dryness Eg medical oxygen has 67parts per million or less of water contamination.
The lung alveoli requires air reaching it to be at 100% humidity, that is dew point.
Can you see the mis-match?
Oxygen is manufactured by stripping air of moisture. Oxygen is a product of air NOT a constituent of air.
There is no wild/natural oxygen in air. Oxygen becomes nitrogen or black oxygen with the addition of carbon particles to become non-flammable oxygen. I have a link to a brilliant demonstration of this on my stack, a home oxygen concentrator is used.
The air we breathe has zero oxygen or nitrogen or the other 1% of ‘gases’. This is a schooled daze program.
The lungs are responsible for re-hydrating the red blood cells as they pass through the alveoli capillaries with salt water. The red blood cells are salt water carriers. The saline intravenous drip rehydrates red blood cells as they pass through the fluid. The saline IV is a hospital's no 1 remedy for very good reasons.
The insult that causes respiratory dis-stress is dehydration. It’s seasonal because cold air holds the least moisture and indoor room air often dries out with heating.
The dry mucosa must re-establish itself and the production of mucus goes into overdrive. The mucosa requires salt and moisture and it will move both from any bodily reserves. This causes pain as the extraction process goes into motion.
Now you know why the old remedies are successful.
Salt water gargles, nasal irrigations/inhalations and chicken soup / bone broth soups.
Sanatoriums were built along coastlines to take advantage of sea spray because it was known to heal injured lungs.
It is time we reclaimed the knowledge of hydration and healing.
Hydration equals salt plus water.
Healing begins with hydration.
Oxygen’s toxicity is directly related to its power to dehydrate. Reactive oxygen species ROS describes damage due to dehydration.
Oxygen on release from a container will extract moisture from its surroundings to become air, its natural state. Oxygen released inside the respiratory tract extracts moisture from the mucosa and the delicate alveoli causing dehydration. This can kill.
Oxygen is a prescribed drug. It is primarily prescribed for the terminally ill. Palliative care is not kind. Notice the portable oxygen tanks have no mitigation for oxygen’s known dryness. Humidity is monitored in anaesthesia and mechanical ventilation. Even CPAP machines have humidifiers included. But the terminally ill are left with straight oxygen, to dry up inside, to endure immense suffering, so they wish for their own demise.
We all need to comprehend the difference between air and oxygen. Read the material safety data sheets for oxygen and nitrogen. Both have unconsciousness and not breathing listed under inhalation.
How does salt restriction lead to heart dis-ease and fear based reactionary thinking? I link dehydration with the adrenals. Dehydration or low salt or hyponatremia are the same condition. Dehydration is an emergency. All emergencies are managed by the adrenals. All the adrenocortical hormones are released, not just aldosterone. This brings the FIGHT/FLIGHT/FREEZE response. It prevents critical thinking and it causes stress intolerance. This makes people very easy to manipulate.
I assert learning the symptoms of dehydration or low salt is necessary so we can identify and remedy with salt plus water.
Hydration is necessary for healing. Hence with salt we are a robust healthy lot. Without salt due to the fraudulent salt restriction directives, sickness increases. Just compare any dis-ease statistics from 1970 to today and see the growth. This growth is also the growth of big pHARMa and why it has been able to co-opt govern minds.
There is more, I tip over a few sacred cows, get ready to revisit all you think you know.
My articles are found by clicking on my blue icon.
Please read my articles and notes and ponder.