

Ending Childhood Pneumonia #3

Recap from our last update:
We scoped down to India - because the infrastructure (in terms of internet, roads, economy, and electricity) was better than other potential locations.
We scoped down to focusing on vaccine for prevention, and determined India’s need for the PCV vaccine for it’s population aged <5.
We identified that one of the most pressing parts was the actual transportation vaccines to the correct location without facing temperature damage.
Update: We’ve identified that the wasting of PCV vaccines are relatively low, hence, not the most pressing issue.
Our goal = how do we end preventable deaths from childhood pneumonia?
Here’s what you’ll learn from this update:
The Vaccine Pipeline
The Status Quo of Vaccine Storage and Distribution in India
Gaps identified in Administration & Last Mile Delivery
Our next steps
The Vaccine Pipeline
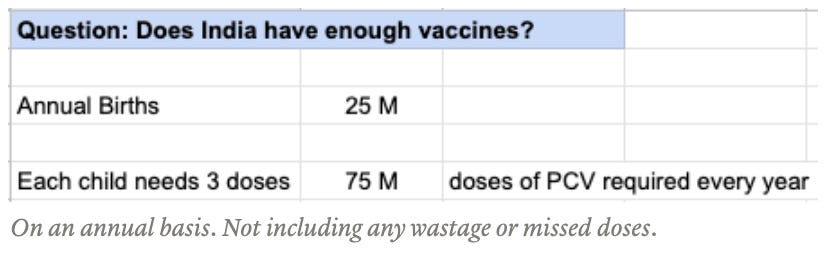
For all children under the age of 5, we’ve roughly estimated the need to be about 300 million doses.
India is a Gavi eligible country (eligible for vaccine subsidy from Gavi, the Vaccine Alliance). Gavi, UNICEF, and the government of India evaluate and calculate the required number of vaccines on an annual basis.
As of Nov 2021, Gavi is providing 60M PCV vaccines, and the Serum Institute in India is providing 9M vaccines with their novel Pneumosil vaccine, which was recently FDA approved. Over the next few years, the Serum Institute will continue to scale up this production.
Original thought: India does not have enough vaccines to vaccinate their population of <5 children by a significant margin → this is a major bottleneck.
Concluding thoughts: Although this is a problem, Gavi, UNICEF and the government produce estimates based on they can afford + what the immunization system can handle.
Even if we get an additional 300 M+ vaccines (enough to immunize all children <5 in India) - does this mean that having this supply will actually translate to immunizations? Not really, because the other parts of the pipeline also need to be dealt with.
India has been ramping up their immunization program over the last while and will continue to do so in the future. Although this is a problem, it’s not the biggest bottleneck in pneumonia vaccinations.
Storage + Distribution of Vaccines

The biggest risk with vaccines and cold chain management is a risk with temperature excursions, which reduce the potency and effectiveness. The PCV vaccine needs to stay within 2-8 degrees celsius. There are two types of temperature damage:
Opened vial - very low (0.24%): Occurs at administration point. The PCV vaccine is packaged in vials with 5 doses, but because of the UN’s multi-dose vial policy, unused doses can be reused for up to 28 days after, as long as no temperature damage occurs. Because of the MDVP, opened vial wastage is nearly non-existent.
Unopened vial - mostly low: Occurs when getting from manufacturing level to the administration point at clinics. Surprisingly, this is also relatively low.
💡 Note: UNICEF’s National Wastage Assessment in India stated that there were 0 PCV vaccines wasted in the unopened vial stage, which we (along with people we’ve talked to) believe to be is wrong, and perhaps attributed to a small sample size. The report stated that of 1.1 billion doses of all antigens (PCV + others like JE, measles, TT, DPT, BCG, etc), 7400 doses were wasted at the unopened vial stage.
The statistic of 0.24% of PCV vaccine at the opened vial stage is also from the same wastage report and also has a probability of being unrepresentative of the real numbers.*
Our thoughts: Although the numbers are not as low as the report states, we believe that cold chain management is not the biggest barrier in India’s PCV adoption. Here’s why:
There are a lot of vaccines within India’s immunization program, and a limited amount of space (during transport + storage) for individual type of vaccine, which means that there’s less space for the PCV vaccine.
Because of the roll-out of the pentavalent vaccine, we no longer need space for BOTH the DPT and Hep B vaccines, creating more space for PCV(+ other vaccines)
Along with this, India conducted an assessment of their cold chain infrastructure (pre-COVID), and launched eVIN (electronic vaccine intelligence network) in all 28 states. The goal of eVIN was to digitize information on vaccine stocks and temperature management.
Over 29 thousand vaccine storage centres or cold chain points are live on eVIN and regularly use the platform to perform daily transactions with respect to vaccine and logistics management.
Facilitated real-time monitoring of storage temperatures by installation of nearly 25,000 temperature loggers.
Supported a vaccine availability rate of over 99% at all cold chain points
Achieved over 80% reduction in instances of vaccine stock-outs and ensured improved availability of adequate and potent UIP vaccines to all targeted children and pregnant women.
Systemized processes by initiating corrective action to revise target population for cold chain points that were earlier out-of-sync, improve vaccine storage infrastructure and encourage effective planning and distribution.
India’s eVIN is considered a major feat and is actively being deployed in other countries (like Malawi, Sudan, Afghanistan, and Indonesia).
Takeaway: Although the platform is not perfect (there are gaps on the usability side with digital literacy), eVIN was a major step forward in the cold chain management system. Because of COVID, India was forced to accelerate and scale up eVIN, which had downstream positive impacts on their immunization program.
Administration + Last Mile Delivery
At this point, if the vaccines are getting to the clinics, what are the gaps to getting children vaccinated?

The incentive for parents to get their children vaccinated just isn’t high enough.
Not understanding the true negative consequences of vaccine preventable diseases + the benefits of vaccines
Fear of vaccines or adverse events following immunization (AEFI)
Vaccination sites are located too far. Mothers must miss a day of work to immunize their child, and when in poverty, every dollar makes an impact.
Do I go to work today and feed my family tomorrow, or do I take my child to get immunized for a disease that may or may not occur in the future, and forgo the day’s earnings?
How Far Must a Mother Travel for Vaccinations?
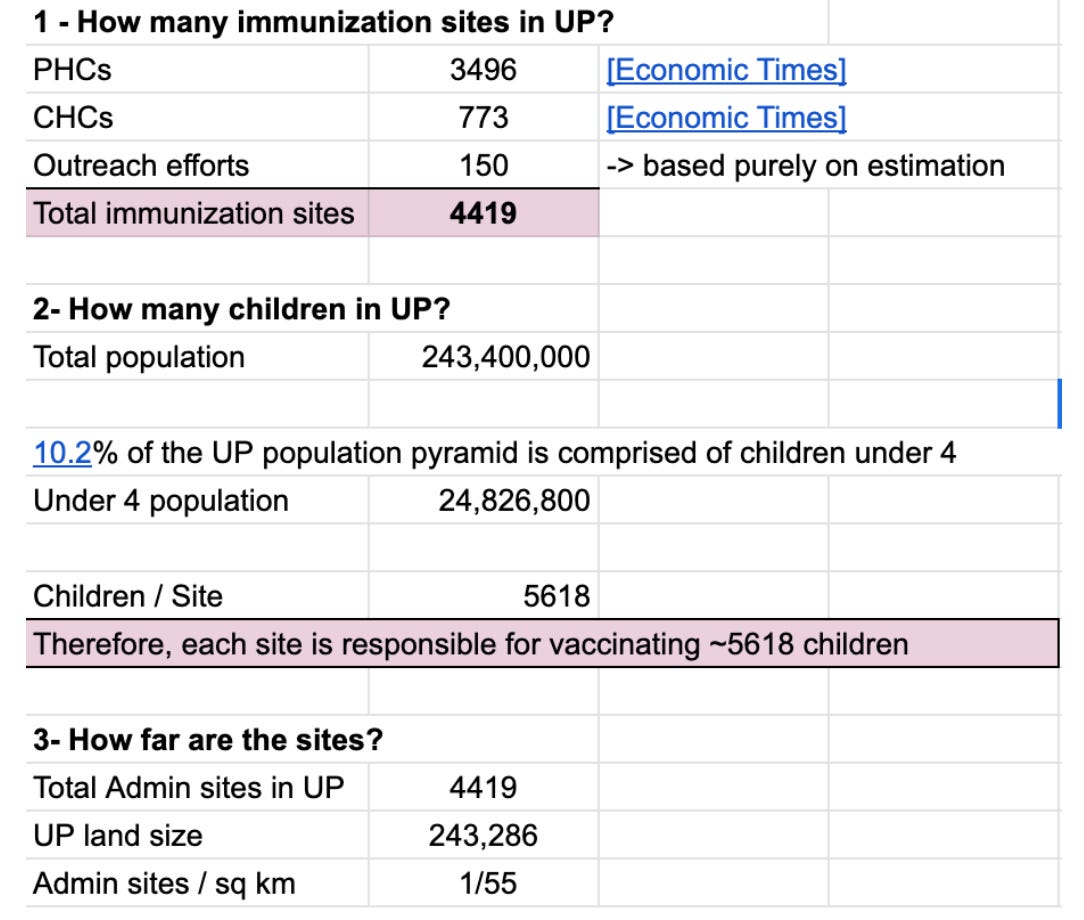
Therefore, there is one administration site for every 55 km. This is a high number, and to account for any errors, the final number we're using is 1 administration site for every 30 km.
Note that immunizations are not a 'one and done' situation - there are many vaccines that need to be administered at many different times, which means that the parents (typically the mother), needs to travel frequently to get all immunizations, especially when the child is <1 yrs old.
In the state that we’re focusing on, Uttar Pradesh, nearly 40% of the population is considered multidimensionally poor (based on health, education, and living standards metrics), and we estimate their daily income to be $1.45.
💡 The biggest gap and opportunity for impact lies in the last mile administration part of the pipeline.
The most difficult part, especially for rural areas is getting the children to the vaccines ⇒ Instead of getting the children to the vaccines, is there any way that we could get the vaccines to the children instead?
Where are we right now? + Next Steps:
We’re currently learning more about the administration portion of the pipeline. Specifically, developing hypotheses on how to increase the scale of Mobile Vaccine Clinics in a manner that is economically incentivized. We will be working with various mentors to validate our hypotheses.
Shoutouts:
Arun: thank you for providing us with incisive insights to help identify gaps in our knowledge and our next steps. We’re looking forward to many more conversations in the future :)
Our Asks:
We’re currently looking for connections to anyone working in vaccine distribution, cold storage, pneumonia vaccines, healthcare in developing countries, or pneumonia organizations in general.